
In the 23 years since the first approval of a targeted therapy (Gleevec)1 in chronic myeloid leukaemia, the implementation of precision medicine across haematological malignancies has been dramatic but fragmented.
Patients with acute or chronic leukaemia can now benefit from several therapies targeted to the specific genomic aberration that defines their subtype of disease, with a number more in advanced stages of development (see the Part 1 on AML here). In contrast, there is not a single approved precisely targeted therapy for patients with multiple myeloma (MM), an incurable condition which can cause abnormal plasma cells to form tumours within the body and produce unneeded plasma proteins.2
Figure 1: Predicted global incidence of multiple myeloma in 2020.
News of potential new treatment modalities for MM, including CAR-T therapies and bi-specific antibodies, was abound at this year’s ASH meeting. However, as yet these prospective therapeutics are not being accompanied by biomarker testing which would aid in identifying which MM patients would most likely benefit from their use, or indeed be most susceptible to their possible toxicities.
Through the routine use of comprehensive FISH panel testing at diagnosis it is possible to distinguish between subgroups of MM patients which may have widely varying prognoses, and in some cases be associated with differences in underlying disease biology. The relevance of these diagnostic cytogenetic biomarkers has not yet been shown for targeting newer classes of biological therapy in MM.
However, there is promising news of their potential utility in the identification of patients who may benefit from the next generation of a well-established drug class used in treating a number of haematological malignancies, BCL-2 inhibitors.
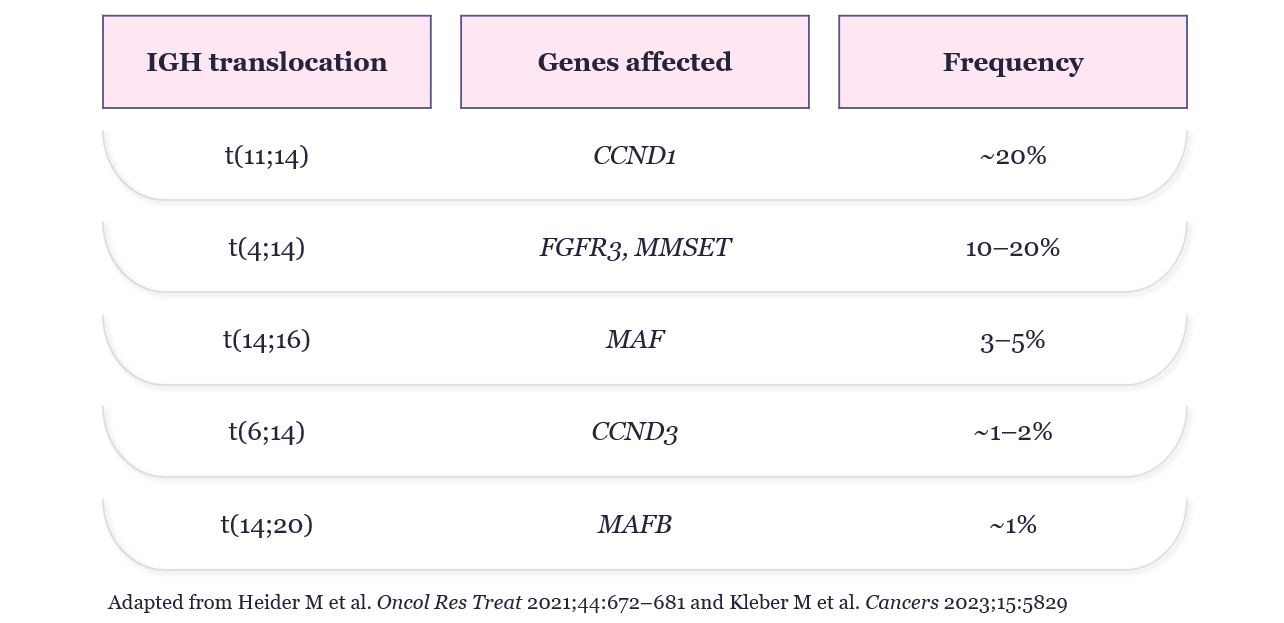
Figure 2: Common translocations in patients with newly diagnosed multiple myeloma4,5
For many years it has been recognised that the 20% of patients whose MM is defined by t(11;14) translocations are more likely to over express the anti-apoptotic protein BCL-2, a key driver of malignant cell proliferation.5 Thus, t(11;14) was identified as a biomarker for patients who may benefit from BCL-2 inhibition but was followed by the recent disappointment of venetoclax, a first generation BCL-2 inhibitor failing in a Phase 3 trial of t(11;14) positive MM patients.6
The MM research and clinical community remains convinced that the BCL-2 pathway could and should be targeted in these patients. This confidence was reinforced by early Phase 1b/2 results presented at the ASH 2023 meeting of second generation BCL-2 inhibitors, which may have higher potency and/or better safety profiles. In particular, results presented from the Phase 1b/2 study of sonrotoclax in t(11;14) patients showed promising rates of response, albeit in a small dose escalation cohort.7
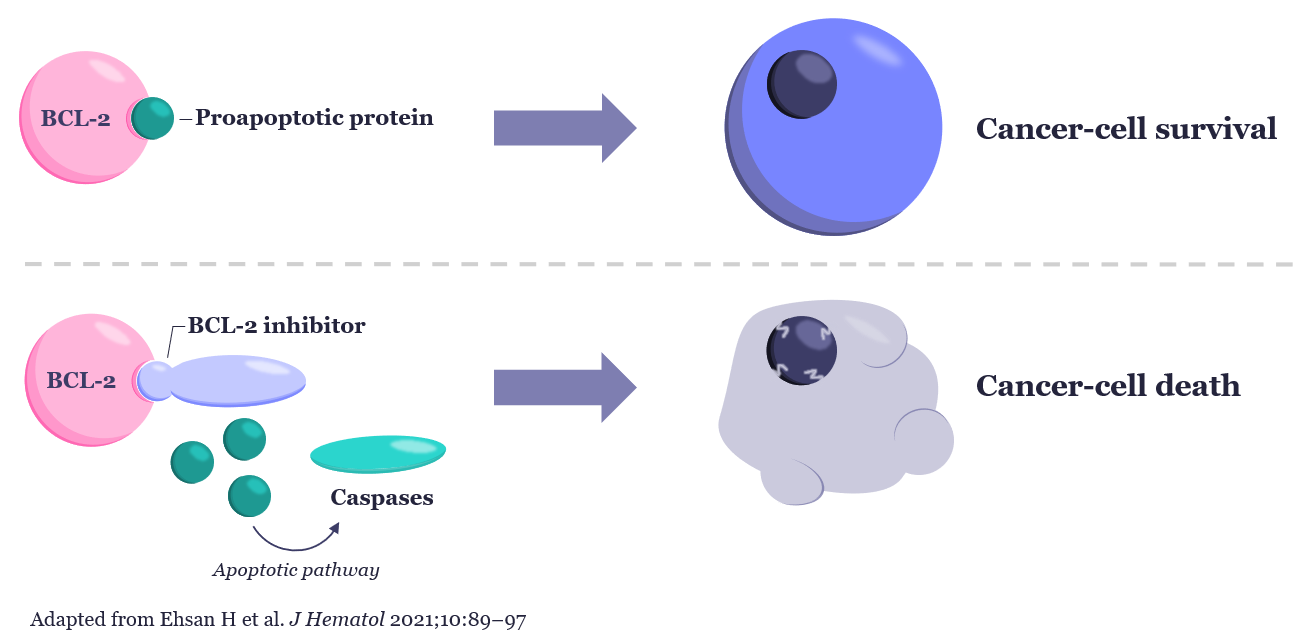
Figure 3: The mechanism of action of BCL-2 inhibition in cellular apoptosis8
For patients with t(11;14) positive malignancies there is certainly hope that better, more targeted therapies may be on the way in the coming years. Of course, there is further work to be done in randomised, controlled late stage trials to determine the efficacy of second generational BCL-2 inhibitors. Nevertheless, patients and clinicians can be reassured that diagnostic companies, including OGT and our partners in cytogenetics laboratories around the world, are well placed to support future development and implementation requirements.
OGT is committed to continuous improvement of our CytoCell® IVD FISH probe panels, including multiple myeloma panels that detect t(11;14) translocations, to ensure they remain compliant with the most stringent regulatory expectations, including IVDR, and we are ready to support their use in both clinical trials and, in the future, as companion diagnostics.
See how you can leverage OGT’s clinical expertise to ensure you maximise your IVDD and IVDR cytogenetics workflow efficiency here: www.ogt.com/ivdr
Note: IVDR-approved probes are only available in Europe and selected other countries.
Call +44 (0)1865 856800 Email contact@ogt.com
Send us a message and we will get back to you
 Visit USA site
Visit USA site Visit Canada site
Visit Canada site